
Description
Buy Avanafil Powder: Complete Guide to Uses, Side Effect and Comparisons
Medical disclaimer: The information below is educational and not a substitute for professional medical advice. Avanafil is a prescription medication. Always consult a licensed clinician to confirm it’s appropriate and safe for you.
What is Avanafil? (and its regulatory status)
Avanafil is a modern, highly selective phosphodiesterase-5 (PDE-5) inhibitor that enhances penile blood flow during sexual stimulation, improving erection quality and maintenance. In the US it’s marketed as Stendra® (FDA-approved in 2012); in the EU/UK/AU it’s Spedra® with similar usage and dosing—see official product docs: FDA Stendra label and EMA Spedra SmPC. FDA Access Data+1
In June 2024, the FDA listed the first generics of Avanafil (50/100/200 mg), improving affordability and access; several manufacturers have since announced launches or availability updates (FDA First Generics list; Camber launch note). U.S. Food and Drug Administration+1
For high-level patient-friendly overviews, see MedlinePlus ED aftercare page (Avanafil listed alongside other ED pills) and Australia’s consumer leaflet Spedra CMI (PDF). MedlinePlus+1
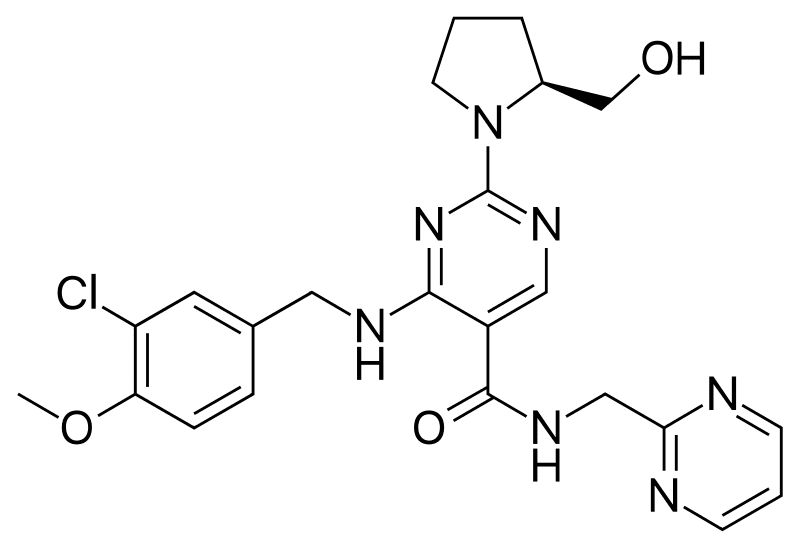
Product information
Synonyms TA-1790
Formal name 4-[[(3-chloro-
Cas number NA
Formula C23H26ClN7O3
Molar Mass 483.96 g·mol−1
Formulation Powder, Crystalline Solid
Solubility
- DMF: 20 mg/ml
- DMSO: 20 mg/ml
- DMSO:PBS (pH 7.2) (1:20): 0.05 mg/ml
Shipping & Storage Information
TA-1790, Avanafil
How Avanafil works (in plain English)
During sexual arousal, nitric oxide in penile tissue raises cGMP, relaxing smooth muscle and allowing blood to fill the corpora cavernosa. PDE-5 is the enzyme that breaks down cGMP. Avanafil selectively inhibits PDE-5, sustaining cGMP and improving erectile function only in the presence of sexual stimulation. This mechanism is consistent across the class and reflected in both US labeling and EU SmPC.
Major urology guidelines recognize PDE-5 inhibitors (including Avanafil) as first-line therapy for most men with ED after shared decision-making — see the AUA ED Guideline and the 2018 Journal of Urology guideline paper. American Urological Association+1
Onset, duration, and what to expect in real life
One of Avanafil’s key advantages is speed. In a randomized, double-blind, placebo-controlled J Urol study, researchers observed successful intercourse at ~15 minutes post-dose in a subset of men — a finding often cited to explain Avanafil’s “on-demand” convenience (full PDF of the trial).
Most men see optimal effect by 30 minutes, with benefits lasting about 6+ hours (individual results vary). Heavy/high-fat meals may delay onset slightly; alcohol ≥ 3 units may increase dizziness or hypotension, so moderation is wise — these points are spelled out clearly in the FDA label and consumer leaflets.
For people who prefer a longer “window”, tadalafil (another PDE-5 inhibitor) can last up to 36 hours or be taken daily. Your clinician can help you choose based on timing preferences, tolerability, and medical history (see AUA guideline for therapy selection principles).
How Fast Does Avanafil Work?
Avanafil is known for speed. In randomized research, a subset of men achieved successful intercourse ≈15 minutes after dosing, with many experiencing clear benefit by 30–60 minutes when sexual stimulation is present (time-to-onset study, J Urol). Practically, you can expect a functional window of 6+ hours, tracking with avanafil’s ~5-hour half-life (per the FDA label), though most couples find the first 2–3 hours the most reliable.
Food won’t “block” avanafil, but heavy/high-fat meals can slow onset; alcohol ≥3 drinks raises dizziness/low-BP risk and can undermine performance (label guidance). To get consistent results, start with 100 mg 15–30 minutes pre-sex, keep meals lighter, go easy on alcohol, and prioritize foreplay.
If 100 mg is close but not quite there, clinicians may consider 200 mg (still once daily max); if side effects bother you, 50 mg with earlier timing often works better. Never combine avanafil with nitrates or riociguat, and review CYP3A4 interactions with your prescriber. Read our full guide for practical timelines, optimization steps, and safety checkpoints.
Read more: How Fast Does Avanafil Work
Dosing: how to take Avanafil safely
Most adults start at 100 mg, taken 15–30 minutes before sex; then titrate to 50 mg (if side effects) or 200 mg (if effect is inadequate), with a maximum of one dose per 24 hours. You can take avanafil with or without food, but heavy/high-fat meals may delay onset; plan earlier dosing or keep meals lighter.
Keep alcohol light (≤2 drinks) — ≥3 increases dizziness/low-BP risk and can undermine erections. For a faster start, set up the first few doses carefully (lighter meal, minimal alcohol, good stimulation) before deciding to escalate from 100 mg to 200 mg.
Never combine avanafil with nitrates or riociguat/vericiguat, and avoid strong CYP3A4 inhibitors; if you’re on a moderate CYP3A4 inhibitor such as erythromycin, diltiazem, verapamil, or fluconazole, follow label dose limits (U.S.: ≤50 mg once/24 h; EU: ≤100 mg once/48 h).
If you’re taking an alpha-blocker, be stable on it first and start avanafil 50 mg, monitoring for dizziness. For men who want an all-day window or daily flexibility, discuss whether tadalafil is a better fit. See our full dosing guide for step-by-step titration and safety checkpoints.
Read more: Full Dosing Guide →
-
Starting dose: 100 mg once, taken 15–30 minutes before sexual activity.
-
Adjustments: Increase to 200 mg or reduce to 50 mg based on effect and tolerance.
-
Frequency: Do not exceed one dose per day.
-
Food: With or without food (heavy/high-fat meals can slow it a bit).
-
Alcohol: Avoid excess alcohol (≥3 drinks can worsen side effects/low BP).
All of the above come straight from the FDA Prescribing Information and the EMA SmPC.
Not much is known about the pharmacological and toxicological properties of Avanafil. Usage of this Chemical should be for research and forensic purposes only.
Special cases (always ask your prescriber):
-
Strong CYP3A4 inhibitors (e.g., ketoconazole, ritonavir, clarithromycin): avoid; they can dramatically raise Avanafil levels (FDA label).
-
Moderate CYP3A4 inhibitors (e.g., erythromycin, diltiazem, fluconazole, verapamil): your clinician may cap at 50 mg once daily.
-
Renal/hepatic impairment: mild-moderate impairment often doesn’t need dose changes, but severe hepatic impairment is not recommended; see specific tables and guidance in the 2018 label and the 2022 label. FDA Access Data+1
-
Age ≥65: No mandatory adjustment solely based on age, but individual sensitivity can vary; titrate under clinician direction.
Who should not take Avanafil (and when to pause)
Absolute contraindications (do not use):
-
Nitrates (nitroglycerin, isosorbide) or guanylate cyclase stimulators (e.g., riociguat) → risk of profound hypotension.
-
Known hypersensitivity to Avanafil or excipients.
These are explicitly listed in the FDA Stendra label and EMA Spedra SmPC.
Use with particular caution / seek clearance:
-
Recent MI or stroke, unstable angina, serious arrhythmias, or conditions where sexual activity is inadvisable.
-
Alpha-blockers (BP/prostate meds) — additive BP-lowering; may need spacing and stable dosing.
-
History of NAION or retinal disorders; anatomical penile deformities; predisposition to priapism (e.g., sickle cell disease).
Risk-benefit and monitoring guidance are covered in major guidelines and the FDA label; clinicians will personalize decisions (AUA Guideline).
Avanafil & Heart Safety
For men with stable cardiovascular disease, sexual activity is typically safe after clinical evaluation, and avanafil can be considered if you are not on nitrates or GC stimulators. The U.S. label requires a ≥12-hour window before emergency nitrates after avanafil; alpha-blockers call for a 50 mg start and caution with alcohol.
After uncomplicated MI, many men can resume sex ~1 week post-event if they can perform moderate activity without symptoms—always confirm with your cardiologist. Observational studies suggest no increase in cardiac events with PDE-5 inhibitors and possible reductions in mortality, but randomized trials are still needed. See full guidance in our Avanafil and Heart Safety.
Interactions that matter
The most important rule is safety. Avanafil must not be combined with nitrates or guanylate cyclase stimulators (e.g., riociguat, vericiguat) due to dangerous blood‑pressure drops; if emergent nitrates are needed after avanafil, clinicians generally wait ~12 hours and monitor closely.
- Absolutely avoid combining with nitrates or riociguat.
Strong CYP3A4 inhibitors (e.g., ketoconazole, ritonavir, clarithromycin, itraconazole, atazanavir) are contraindicated; moderate inhibitors (e.g., erythromycin, diltiazem, fluconazole, verapamil, aprepitant) require dose limits (U.S.: ≤50 mg once/24 h; EU: ≤100 mg once/48 h).
- Strong CYP3A4 inhibitors can dramatically raise Avanafil levels — avoid unless instructed otherwise.
- Moderate CYP3A4 inhibitors may require dose limitations (often 50 mg max) and careful spacing.
On alpha‑blockers (tamsulosin, doxazosin, etc.), be stable first and start avanafil at 50 mg; both are vasodilators, so lightheadedness can occur. Keep alcohol light (≥3 drinks raises risk) and avoid grapefruit around dosing (can raise avanafil levels). For patient‑friendly reminders, see MedlinePlus.
- Alpha-blockers (e.g., tamsulosin, doxazosin) can add to BP-lowering — your prescriber may adjust timing/dose.
All of these are detailed in the FDA label’s interactions section (and summarized by payers/formularies, e.g., Health Net policy PDF).
Read more: Full Interactions Guide →
Side effects & safety signals
Avanafil’s most frequent side effects are headache, flushing, nasal congestion, back pain, and dizziness; they’re usually mild and improve with hydration, lighter meals, and dose/timing adjustments. Red‑flag symptoms needing urgent care include priapism (erection >4 hours), sudden vision loss (possible NAION) or severe visual changes, sudden hearing decrease/loss, and fainting or severe dizziness.
This profile aligns with class-wide warnings and appears in both the FDA label and EMA SmPC.
Visual “blue-tinge” symptoms are linked to PDE-6 activity and appear less frequently with Avanafil than with sildenafil or vardenafil (comparative selectivity noted across pharmacology reviews and clinical experience; see NICE evidence summary for comparative outcomes).
Risk rises with nitrates/riociguat (contraindicated), strong CYP3A4 inhibitors (e.g., ketoconazole, ritonavir, clarithromycin, itraconazole), heavy alcohol (≥3 drinks), grapefruit near dosing, and alpha‑blockers if you’re not yet stable.
Safer use starts with the lowest effective dose, 15–30 min pre‑sex, minimal alcohol, no grapefruit, and coordination with your clinician for interacting meds. Turn to our dosing, interactions, and onset guides for optimization, and read official labeling for complete warnings.
Read more: Full Side Effects Guide →
Avanafil vs other ED medications (choosing what fits your life)
All PDE-5 inhibitors share the same end-goal (support erections during sexual stimulation), but differ in onset, duration, food sensitivity, and side-effect patterns.
| Feature | Avanafil | Sildenafil | Tadalafil | Vardenafil |
|---|---|---|---|---|
| Earliest onset | ~15 min in some men | ~30–60 min | 30–60 min | 30–60 min |
| Duration | ~6+ hours | 4–6 hours | up to 36 h (or daily) | 4–6 hours |
| Food effect | Minimal | High-fat meals slow | Minimal | High-fat meals slow |
| Visual tinges | Lower | Higher (PDE-6) | Rare | Higher (PDE-6) |
Avanafil is an excellent on-demand option when speed & meal-flexibility matter; tadalafil is great for a longer window or daily use; sildenafil remains a reliable, affordable choice for many; vardenafil may suit those who’ve historically done well on it. Treatment choice should reflect your preferences, side-effect tolerance, and medical history — see AUA ED Guideline for general selection principles and shared decision-making. For rapid-onset data specific to Avanafil, see the J Urol trial and complementary evidence in Mayo Clin Proc and PubMed/PMC summaries.
Practical use cases & tips
-
I don’t want to schedule intimacy. Avanafil’s potential ~15-minute onset can be more spontaneous; take it before sexual activity, not daily. (J Urol trial PDF).
-
Heavy dinner date? Because high-fat meals can slow some ED pills, Avanafil’s minimal meal effect can be a plus (compare labels: FDA Stendra vs sildenafil/vardenafil class notes in guidelines).
-
Post-prostatectomy recovery: PDE-5 inhibitors are often part of sexual rehabilitation strategies; Avanafil has label updates reflecting study data in post-RP men (FDA letter noting label updates; see discussion articles like Urology Times for context).
-
Budget-conscious: With 2024 first generics, pricing is improving — consider generic Avanafil where available (FDA First Generics list). U.S. Food and Drug Administration
Buying Avanafil Powder from us: what you get
-
Licensed pharmacy fulfillment (authentic brand or AB-rated generic) buy avanafil powder from us.
-
Pharmacist access to review your meds and check for interactions.
-
Discreet shipping and secure checkout.
-
Fair pricing backed by increased competition since generics arrived (Camber launch note, corroborating the FDA generics list).
Frequently asked questions
How fast does Avanafil work?
Some men can achieve successful intercourse ~15 minutes after dosing, with many experiencing benefit by 30 minutes. Sexual stimulation is required ( Mayo Clin Proc 2012). AUA Journals+1
How long does it last?
Typically ~6+ hours, though response varies. Food has minimal effect versus some older options; heavy/high-fat meals may still delay the start slightly (FDA label).
Can I take it with alcohol?
Limit alcohol; ≥3 drinks can increase dizziness or hypotension. This is a labeled precaution (FDA Patient Info). FDA Access Data
Is there a generic?
Yes — FDA listed first generics (50/100/200 mg) on June 14, 2024; availability varies by region and wholesaler (FDA First Generics). U.S. Food and Drug Administration
Can I combine Avanafil with other ED meds or boosters?
Do not combine PDE-5 inhibitors or stack with nitrates/riociguat. Discuss alpha-blockers and any supplements or recreational substances with your prescriber (see AUA guideline and FDA label).
WARNING This product is not for human or veterinary use.

This product is only available to persons of 21 years old and above.
Hazard statement(s)
| H302 | Harmful if swallowed |
| H315 | Causes skin irritation |
| H319 | Causes serious eye irritation |
| H332 | Harmful if inhaled |
| H335 | cause respiratory irritation |
| H336 | cause drowsiness or dizziness |
| Precautionary statement(s) | |
| P264 | Wash hands thoroughly after handling |
| P280 | protective gloves/protective clothing/eye protection/face protection |
| P305 + P351 + P338 | IF IN EYES: Rinse cautiously with for several minutes. Remove contact lenses, if present and easy to do. Continue rinsing. |
| P337 + P313 | If eye irritation persists: Get medical advice/attention |
| P261 | Avoid breathing dust/ fume/ gas/ mist/ vapors/ spray |
| P271 | Use only outdoors or in a well-ventilated area |
| P304 + P340 | IF INHALED: Remove victim to fresh air and keep at rest in a position comfortable for breathing |
| P312 | Call a POISON CENTER or doctor/physician if you feel unwell |
| P403 + P233 | Store in a well-ventilated place. Keep container tightly closed |
| P405 | Store locked up |
| P501 | Dispose of contents/container to a licensed disposal company |

Reviews
There are no reviews yet.